Lonafarnib / Ritonavir
Hepatitis Delta Virus (HDV) Infection
Lonafarnib/Ritonavir for HDV
Stage
Phase 3 CompletedPositive Pre‑NDA Meeting with FDA
Partnering opportunity
Disease
Hepatitis Delta Virus InfectionPrevalence
100K in the US200K in the EU
Mechanism of Action
Prenylation InhibitorRegulatory Designations
- Orphan in US and EU
- Breakthrough Therapy in US
- PRIME in EU
About Hepatitis Delta Virus
HDV is the most severe form of viral hepatitis
Hepatitis Delta is caused by infection with the Hepatitis Delta Virus and leads to the most severe form of viral hepatitis. HDV occurs only as a co-infection in individuals infected with Hepatitis B Virus (HBV). HDV leads to more severe liver disease than HBV alone and is associated with accelerated liver fibrosis, liver cancer, and liver failure. Approved nucleos(t)ide treatments for HBV only suppress HBV DNA, do not affect HBsAg, and have no impact on HDV.
Lonafarnib is the first and only oral agent in development for HDV
Lonafarnib is a well-characterized, first-in-class, inhibitor of farnesyl-transferase, an enzyme involved in modification of proteins through a process called prenylation. HDV uses this host cell process inside liver cells to complete a key step in its life cycle. Lonafarnib inhibits the prenylation step of HDV replication inside liver cells and blocks the virus life cycle at the stage of assembly.
- Global Phase 3 D-LIVR Study completed
- FDA Breakthrough Therapy designation
- EMA Prime designation
HDV replication and prenylation
After HDV enters a target cell hepatocyte, the genome is translocated to the nucleus where genome replication occurs without the need of any gene products from HBV. An important interaction between HDV and HBV proteins has been shown to depend on the presence of the last 4 amino acids of the large delta antigen, comprising a CXXX box motif, where C represents cysteine and X denotes any other amino acid. This amino acid sequence is required for the protein to be post-translationally modified by farnesyltransferase (FT), an enzyme which covalently attaches a 15-carbon prenyl-lipid farnesyl moiety to the cysteine of the CXXX box. Prenylation of the large delta antigen renders it more lipophilic, promotes its association with HBsAg, and is essential for initiating the HDV particle formation process.The HDV Lifecycle
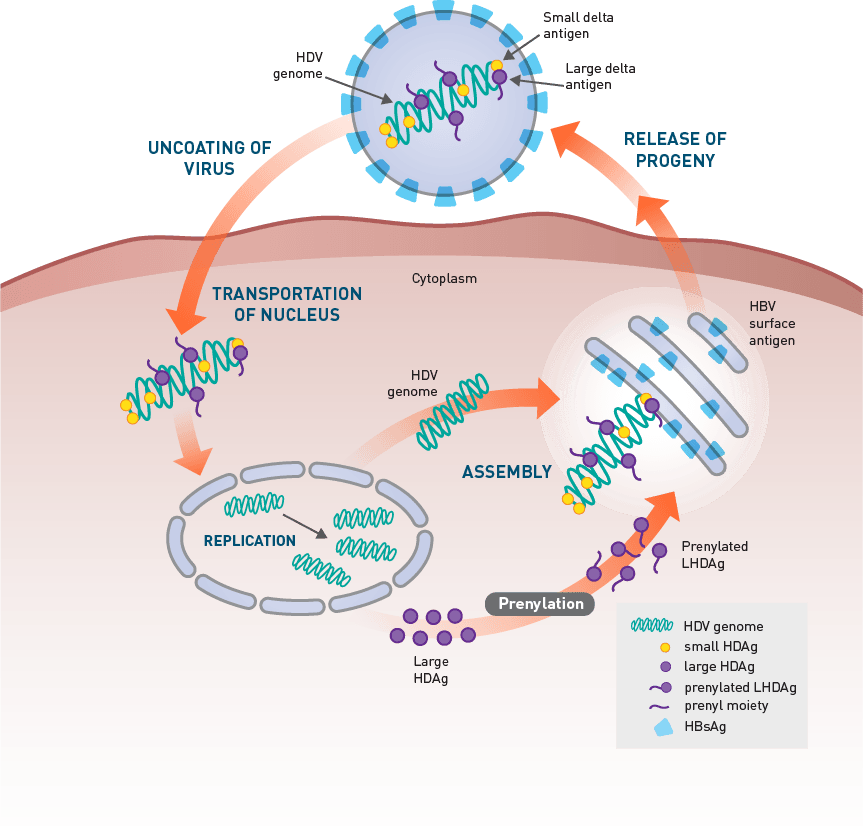
Reference: Elazar M, Glenn JS. Confronting new and old antiviral threats: broad spectrum potential of prenylation inhibitors. In: Torrence PF, ed. Antiviral Drug Discovery for Emerging Diseases and Bioterrorism Threats. Hoboken, NJ: John Wiley & Sons; 2005:249-261.
HDV Prevalence
Hepatitis Delta is a disease with a significant impact on global health, which may affect up to 20 million people worldwide
The prevalence of HDV varies among different parts of the world. Globally, HDV infection is reported to be present in approximately 4% to 6% of chronic Hepatitis B carriers. The prevalence of HDV in patients infected with chronic HBV is even higher in certain regions, including certain parts of Mongolia, China, Russia, Central Asia, Pakistan, Turkey, Africa, Middle East, and South America, with an HDV prevalence as high as 60% being reported in HBV-infected patients in Mongolia and Pakistan.
Globally, HDV infection is reported to be present in approximately 4% to 6% of chronic hepatitis B carriers.
Hdv worldwide prevalence: 15-20 million
(Swipe to interact)

References: 1. Fattovich G, Boscaro S, Noventa F, et al. Influence of hepatitis delta virus infection on progression to cirrhosis in chronic hepatitis type B. J Infect Dis. 1987;155(5):931-5. 2. Calle Serrano B, Grosshennig A, Heidrich B, et al. Comparing the long-term outcome of hepatitis delta and HBV monoinfection: Is HDV-infection really worse? Poster presented at: The International Liver Congress™ 2011; March 31, 2011; Berlin, Germany. 3. Wedemeyer H, Manns MP. Epidemiology, pathogenesis and management of hepatitis D: update and challenges ahead. Nat Rev Gastroenterol Hepatol. 2010;7(1):31-40.
HDV causes the most rapid liver disease progression




70% of HDV-infected patients will progress to cirrhosis within 5 to 10 years and >50% of patients are cirrhotic at diagnosis.
HDV: MOST RAPID PROGRESSION OF DISEASE
50% of HDV-Infected Patients are Cirrhotic at Diagnosis
Lonafarnib in HDV clinical studies
Lonafarnib (LNF) is the first and only oral agent in development for HDV. It is well-characterized and has been previously administered to > 2000 patients in oncology and > 90 children with Progeria. Most common adverse events are gastrointestinal. In our HDV program, we discovered that co-dosing Lonafarnib with ritonavir (RTV), an inhibitor of its metabolism, allows for lower doses of Lonafarnib to be administered with higher concentrations of Lonafarnib in the liver and systemic circulation. Lonafarnib has been dosed in over 400 HDV-infected patients in Phase 2 and Phase 3 HDV studies. Lonafarnib is generally well tolerated. Most commonly reported adverse events to date are diarrhea and nausea. Side effects can be well managed with prophylactic treatment with antidiarrheals and antiemetics. Longest duration of dosing is > 10 years.Learn more about the phase 2 program
- POC Study (Placebo-controlled LNF monotherapy) (N=14)
- LOWR-1 Study (Combination: LNF with RTV or PEG IFN-alfa-2a) (N=21)
- LOWR-2 Study (Dose Finding: LNF + RTV + PEG IFN-alfa-2a) (N=58)
- LOWR-3 Study (QD Dosing: LNF + RTV) (N=21)
- LOWR-4 Study (BID Dose-Escalation: LNF + RTV) (N=15)
About the Phase 3 D-LIVR study
D-LIVR is a global Phase 3 study with the only oral agent in development for HDV. D-LIVR evaluates an all-oral arm of LNF boosted with RTV and a combination arm of LNF boosted with RTV combined with pegylated interferon-alfa-2a (PEG IFN-alfa-2a), with each arm to be compared with a placebo arm (background HBV nucleos[t]ide only), in HDV-infected patients.
STUDY COMPLETE
 Download Presentation
Download Presentation
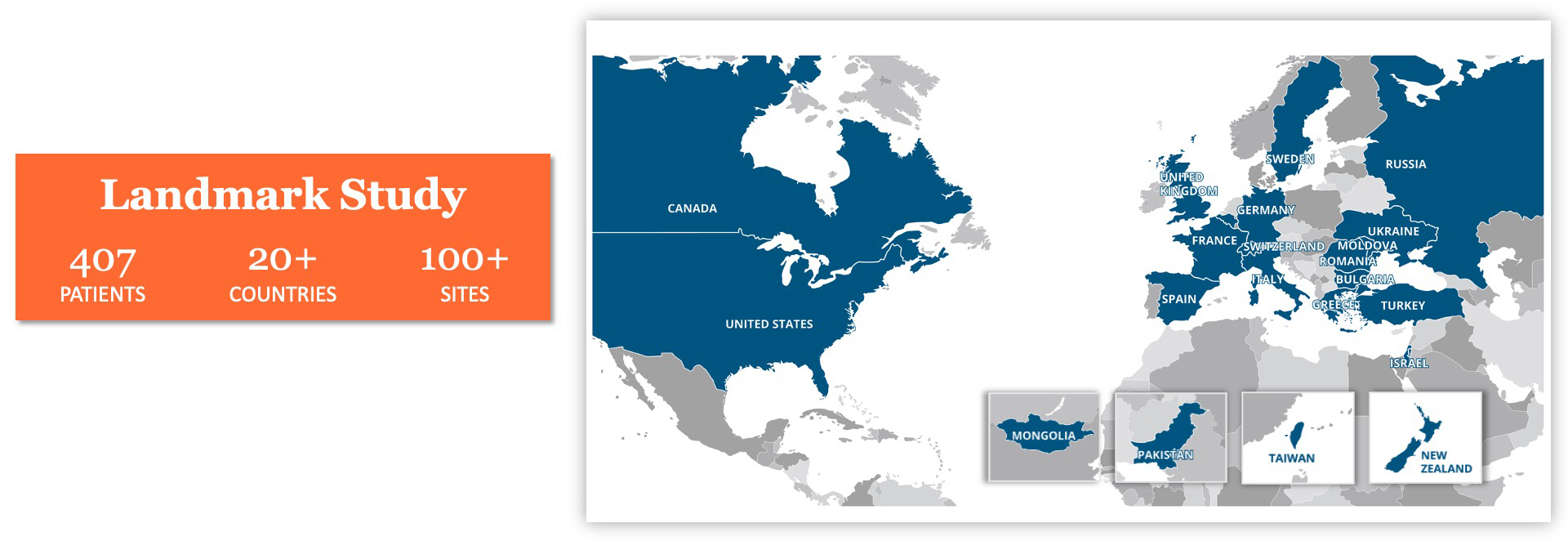
D-LIVR Landmark Phase 3 Global Study
EVALUATION OF TWO LONAFARNIB-BASED REGIMENS AS POTENTIAL FINITE THERAPIES
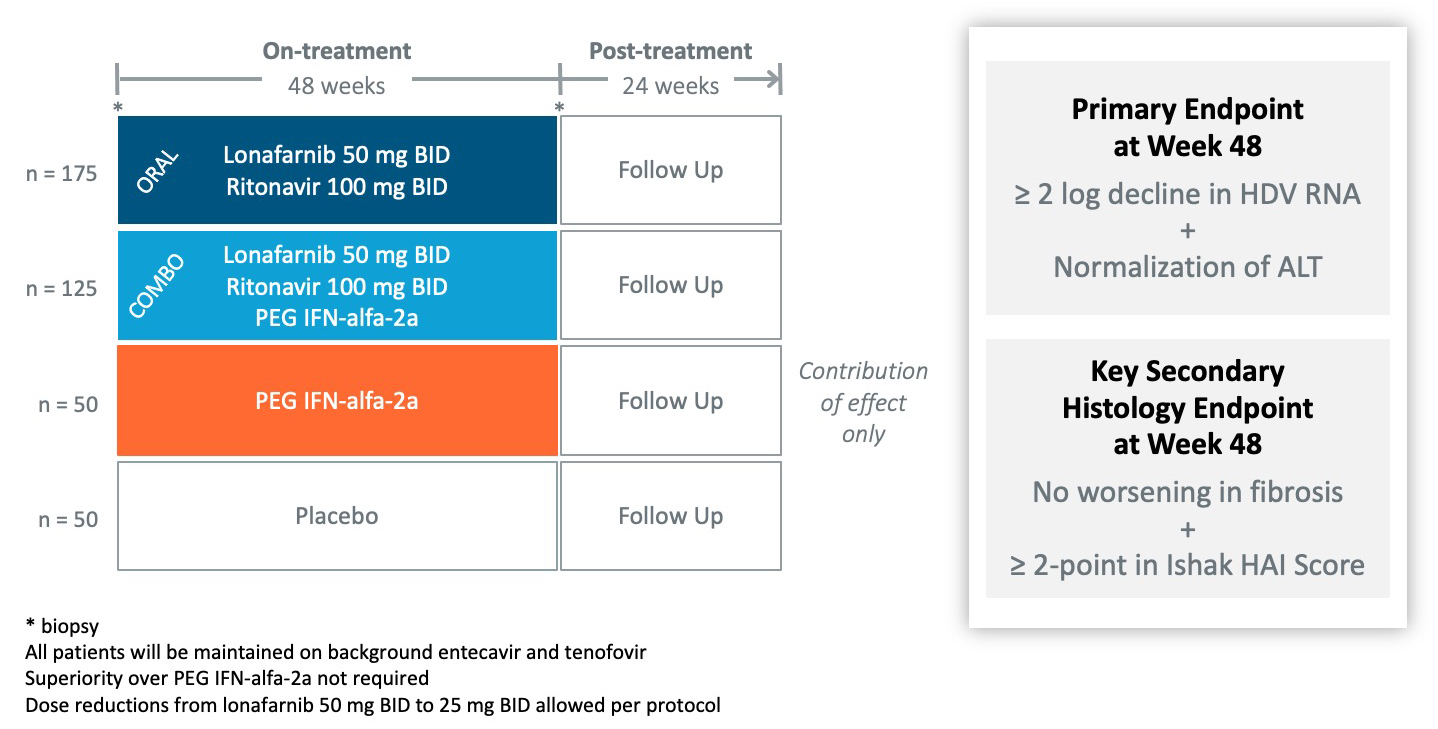
Primary Endpoint Achieved with Significance in BOTH Arms
% PATIENTS ACHIEVING COMPOSITE ≥2 LOG DECLINE IN HDV RNA + ALT NORMALIZATION AT WEEK 48
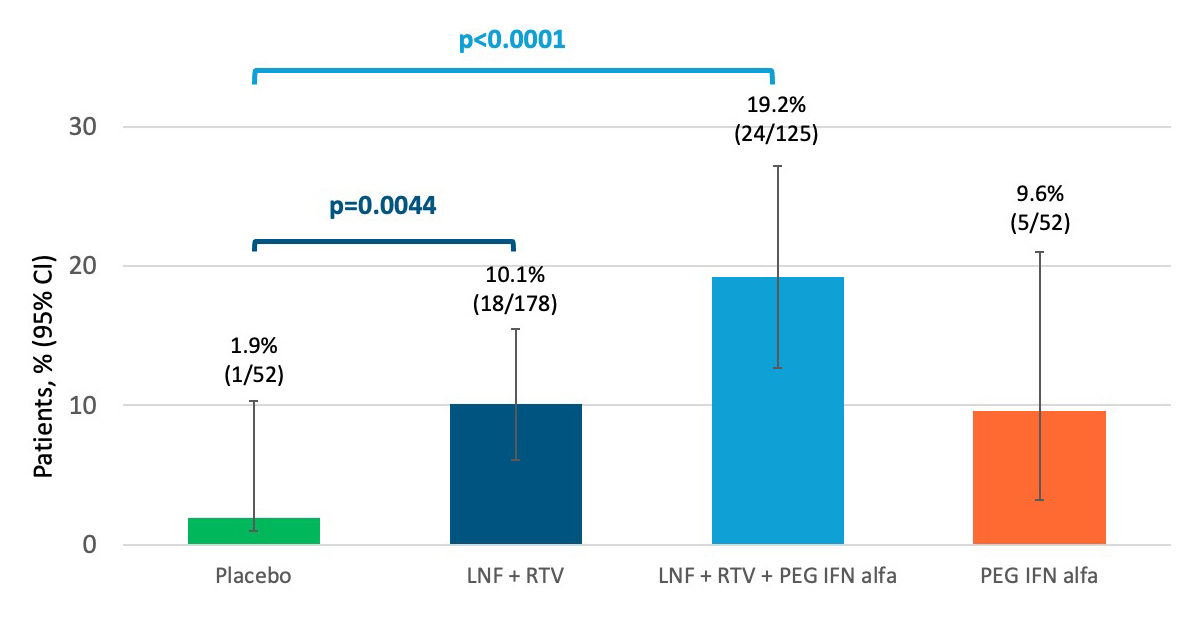
- Importantly, statistically significant improvement in histology observed with the combination regimen
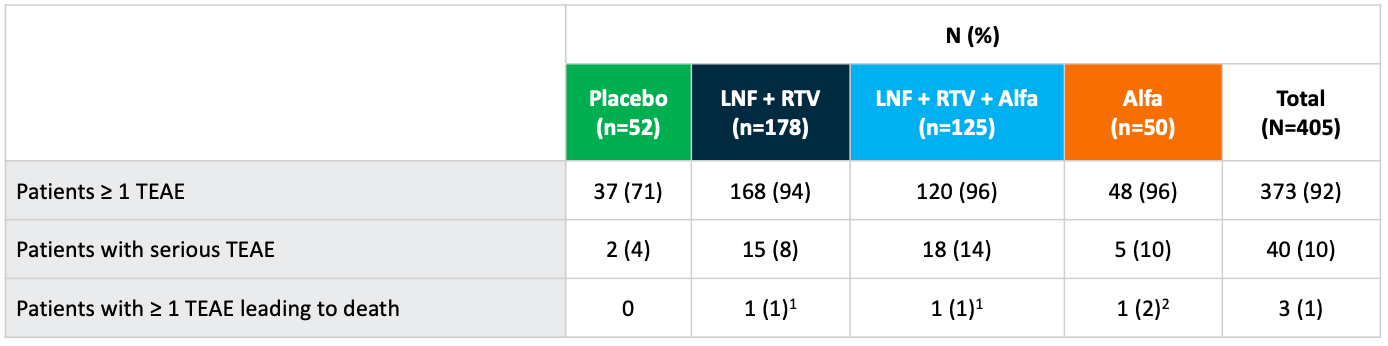
Overall Safety through Week 48
BOTH LONAFARNIB-TREATMENT REGIMENS WERE WELL-TOLERATED
PTWK24 (End of Study) Response for Both Lonafarnib Regimens
COMPOSITE ENDPOINT, RANDOMIZED POPULATION, N=338
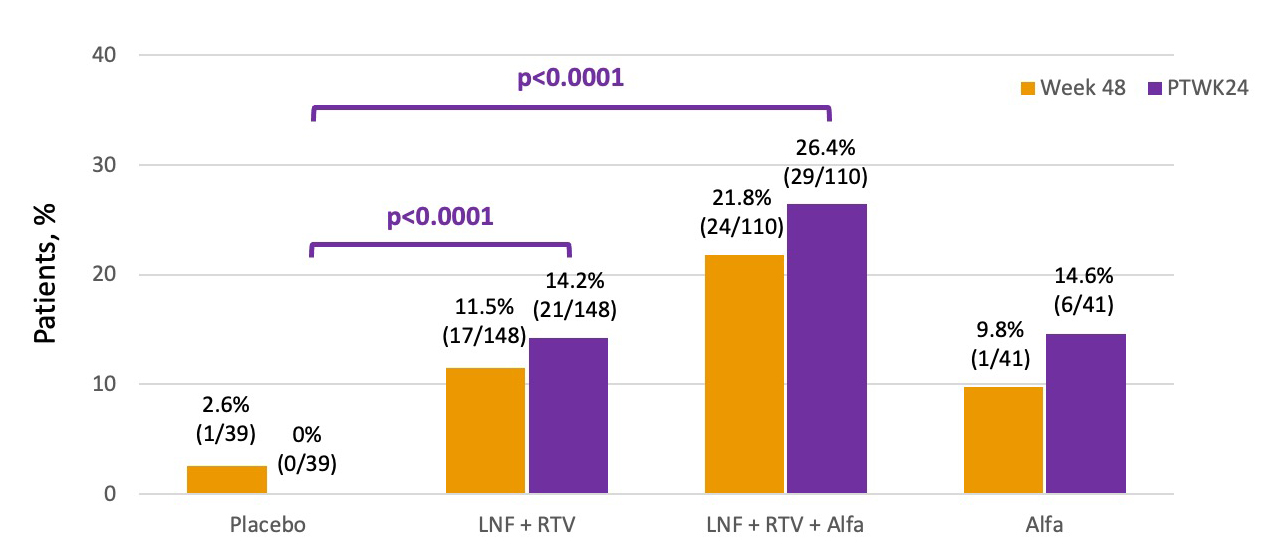
- Increase in response rate post-treatment vs at end of treatment may partially be explained by beneficial flares occurring in approximately 10% of the oral and 20% of the combo arm after stopping treatment.
- Durability of response at 24-week post-treatment suggests that finite therapy may be possible in a subset of patients with chronic HDV.
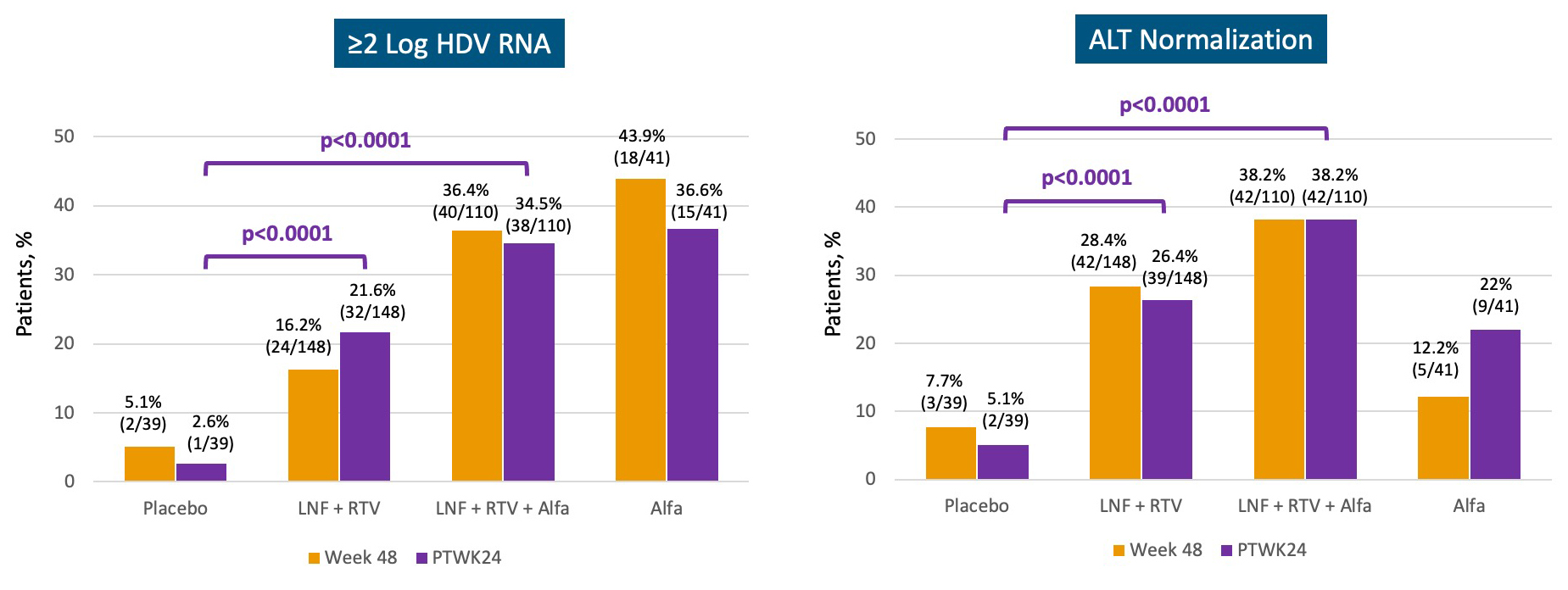
Week 48 vs PTWK24 (End of Study) : Composite Components
RANDOMIZED POPULATION, N=338
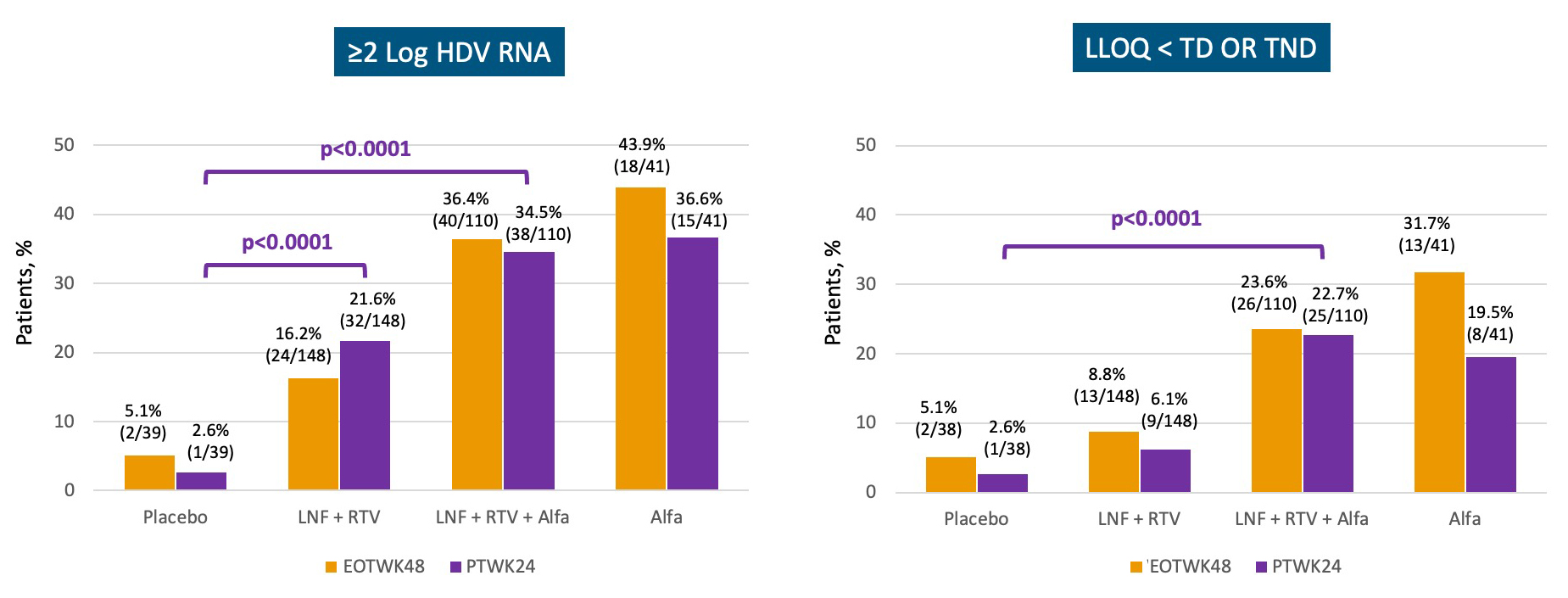
Week 48 vs PTWK24 (End of Study) : Antiviral Response
RANDOMIZED POPULATION, N=338
 For more information, please visit clinicaltrials.gov
For more information, please visit clinicaltrials.gov LONAFARNIB CLINICAL STUDIES IN HDV
- Etzion O et al, “Week 72 Results of the Phase 3 D-LIVR Study, A Randomized Double-Blind, Placebo-Controlled Trial Evaluating the Safety and Efficacy of Lonafarnib-Boosted with Ritonavir with or without Peginterferon Alfa in Patients with Chronic Hepatitis Delta,” Presented at EASL 2023
- Buti M et al. "Strong correlation between HBsAg, ALT and HDV-RNA levels in patients with chronic hepatitis D. Results of Phase 3 D-LIVR study.," Presented at EASL 2022
- Etzion O et al. "Clinical features predictive of cirrhosis in a large cohort of patients with chronic hepatitis delta infection - Insights from the D-LIVR trial," Presented at EASL 2022
- Etzion O et al. "Noninvasive Tests for Detection of Biopsy-proven Cirrhosis In Chronic Hepatitis D Infected Patients are Suboptimal," Presented at AASLD 2020
- Yurdaydin C et al. "Sub-analysis of the LOWR-2 Study Reveals High Response Rates to Lonafarnib in Patients with Low Viral Loads," EASL 2018
- Yurdaydin C et al. "LOWR-2 End of Study," EASL 2017
- Yurdaydin C et al. "LOWR-2 Retreatment," EASL 2017
- Koh C et al. "LOWR-3 End of Study," EASL 2017
- Wedemeyer H et al. "LOWR-4 End of Study," EASL 2017
- Koh C, et al. "Oral prenylation inhibition with lonafarnib in chronic hepatitis D infection: a proof-of-concept randomised, double-blind, placebo-controlled phase 2A trial." Lancet Infect Dis. 2015;15(10):1167-1174.
HDV Severity of Disease
- Calle Serrano B et al. "Comparing the long-term outcome of hepatitis delta and HBV monoinfection: Is HDV-infection really worse?" Poster presented at: The International Liver Congress™ 2011; March 31, 2011; Berlin, Germany.
- Fattovich G et al. "Influence of hepatitis delta virus infection on morbidity and mortality in compensated cirrhosis type B." The European Concerted Action on Viral Hepatitis (Eurohep). Gut. 2000;46(3):420-426.
Prevalance
- Patel EU et al. "Prevalence of hepatitis b and hepatitis d virus infections in the United States, 2011-2016." Clin Infect Dis. 2019;69(4):709-712.
- Franco R et al. "Growing hepatitis delta virus (HDV) infection prevalence in the US: underdiagnosis in foreign-born individuals." Poster presented at: The Liver Meeting 2018: American Association for the Study of Liver Diseases (AASLD); November 9-13, 2018; San Francisco, CA.
- Martins EB, Glenn J. "Sa1486 - Prevalence of hepatitis delta virus (HDV) infection in the United States: results from an ICD-10 review [abstract]." Gastroenterol. 2017;152(5)Suppl1:S1085.
- Chen X et al. "A novel quantitative microarray antibody capture assay identifies an extremely high hepatitis delta virus prevalence among hepatitis B virus-infected mongolians." Hepatology. 2017;66(6):1739-1749.
- Lin HH et al. "Changing hepatitis D virus epidemiology in a hepatitis B virus endemic area with a national vaccination program." Hepatology. 2015;61(6):1870-1879.
- Liao B et al. "Epidemiological, clinical and histological characteristics of HBV/HDV co-infection: a retrospective cross-sectional study in Guangdong, China." PLoS ONE. 2014;9(12):e115888.
- Yan YP et al. "Epidemiology of hepatitis B virus infection in China: current status and challenges." J Clin Transl Hepatol. 2014;2(1):15-22.
- Shen L et al. "Development of a hepatitis delta virus antibody assay for study of the prevalence of HDV among individuals infected with hepatitis B virus in China." J Med Virol. 2012;84(3):445-449
Prenylation
- Bordier B et al. "A prenylation inhibitor prevents production of infectious hepatitis delta virus particles." J Virol. 2002;76(20):10465-10472.
- Glenn J et al. "Identification of a prenylation site in delta virus large antigen." Science. 1992;256(5061):1331-1333.
Long-term Clinical Benefit of Suppressing HDV-RNA
- Wranke A et al. "Antiviral treatment and liver-related complication in hepatitis delta." Hepatology. 2017;659(2):414-425.
- Romeo R et al. "High serum levels of HDV RNA are predictors of cirrhosis and liver cancer in patients with chronic hepatitis delta." PLoS One. 2014;9(3):e92062.
- Heidrich B et al. "Late HDV RNA relapse after peginterferon alpha-based therapy of chronic hepatitis delta." Hepatology. 2014;60(1):87-97.
- Farci P et al. "Long-term benefit of interferon alpha therapy of chronic hepatitis D: regression of advanced hepatic fibrosis." Gastroenterology. 2004;126(7):1740-1709.